
Mastering Emergency Medicine: A Practical Guide: A Comprehensive Guide for MCEM
The following are 11 quality checklist to go through when critically appraise RCT"s
From SGEM
A 45 year old female presents with vertigo and vomiting. The symptoms are worse when she sits forwards.
1. Give 3 features which make a central cause more likely than a peripheral cause.
2. You decide a peripheral cause is most likely. Give the 2 most likely diagnosis.
3. Which test would you use to distinguish between the 2 causes?
4. Explain how you would perform the test?
5. Give 2 classes of drugs that may be used in the chronic treatment of vertigo and examples.
A 75 year old man presents with epistaxis from the right nostril. Bleedining hasn’t settled after pressure for 20 mins. He is haemodynamically stable with BP 170/100
1. Which three drugs, (or classes of drugs) should you ask about?
2. Outline how you would insert a nasal tampon(Rapid Rhino) – you have to explain the procedure to the patient
3. After insertion of the tampon the patient continues to bleed. What does this imply?
4. How would you manage this?
A 2 year old boy presents with a history of coin ingestion. An x-ray is performed.

1. Describe the x-ray
2. How would you manage this patient
A 45 year old female presents complaining of tinnitus and unilateral deafness.

1. What does the scan show?
2. What is the most likely diagnosis?
3. List 3 other lesions that occur in this area
4. Which cranial nerves may be affected by such lesions?
21 year old presents with one week history of sore throat, fever, abdominal pain and recent travel to Spain. He is brought in suddenly after collapsing after a rugby tackle and complaining of abdominal pain.
On examination - Pulse - 110 bpm, BP 100/60, pale, c/o thirst ++, ? jaundiced
Abdomen tender and guarding LUQ
Hb 10, WBC 13, Plt 290, ESR 56, Alb 39, Alk phos 188, ALT 200, Bil 88
1. What is the underlying diagnosis? What complication has occurred?
2. What is the underlying cause and how can it be confirmed?
3. What is the immediate management of this patient?
A 46 year old present complaining of ear ache and discharge. Otoscopy reveals the following.

1. What is the diagnosis?
2. Name 2 groups of patients at increased risk of developing this condition
3. Name 3 organisms implicated in this condition
4. How would you manage the patient?
A 6 year old female presents with fever and ear ache.

1. What is your diagnosis?
2. Name 2 common organisms implicated
3. Give 3 complications associated with this condition
Further reading : NICE CKS
A 25 year old male presents with ear ache and discharge. He has a past medical history of recurrent otitis media. Otoscopy reveals the following.


4. What is the diagnosis?
5. Give 3 causes of the above condition
6. How would you manage this patient in the ED?
1. What is the diagnosis?
2. What is the pathophysiological process associated with this condition?
3. Outline your management in the ED.
4. What is the diagnosis?
5. Give 3 causes of the above condition
6. How would you manage this patient in the ED?
Further read: Patient.co.uk
36 year old female presents complaining of spilling liquids when she tries to drink.

1. Give 4 causes of this presentation
2. Describe the anatomy and how this impacts on presentation of this condition.


45 year old man presents complaining of ear ache and a “lopsided face”.

1. What is the diagnosis?
2. How would you manage this patient?

This page contains guidelines and statements produced by the Royal College of Emergency Medicine"s Quality in Emergency Care (QEC) committee. All links take you to college site or specific download page.
Further links to information and resources on the 2014 Ebola outbreak in West Africa:
Public Health England
European Centre for Disease Prevention and Control
World Health Organisation (WHO)
WHO websiteWHO Global Alert and Response (GAR) - Ebola
The following evidence-based guidelines have been published by GEMNet:
Below is a list of College summaries of clinical guidelines relevant to Emergency Medicine which have been produced by external organisations.
Selected further guidance
A 66 year old male presents to ED with chest pain. His pulse 100, BP 90/58.

The CT1 doctor has commenced Oxygen and given the patient 3 mg buccal nitrate
A 66 year old male presents to ED with chest pain. P100, BP 90/58.
The SHO has commenced Oxygen and given the patient 3mg buccal nitrate
1. What does the ECG show? What is the diagnosis?
2. What would you tell the CT1 to do?
3. List 5 treatment options.
4. Which vessel is involved?


A 61 year old man presents with central chest pain, he is a NIDDM.
He has a troponin I level of <5.

A 61 year old man presents with central chest pain, he is a NIDDM.
He has a troponin I level of <5.
1. Describe the ECG
2. Give 5 components of the TIMI score.
The patient has received aspirin, nitrates and analgesia, give 3 further pharmacological interventions as the patient has ongoing pain.
56-year-old man presents with a 2 hour history of severe central chest pain, vomiting and sweating +++.
On arrival in ED he is seen by a junior doctor who gives Oxygen, gets IV access and an ECG and gives a 5mb buccal tablet and diamorphine 2mg with anti-emetic.
His observations on arrival were P=95/min BP= 169/105.
The doctor comes to ask for your help, as the patient is now more sweaty and confused with a BP 85/45.


56-year-old man presents with a 2 hour history of severe central chest pain, vomiting and sweating +++.
On arrival in ED he is seen by a junior doctor who gives Oxygen, gets IV access and an ECG and gives a 5mb buccal tablet and diamorphine 2mg with anti-emetic.
His observations on arrival were P=95/min BP= 169/105.
The doctor comes to ask for your help, as the patient is now more sweaty and confused with a BP 85/45.
1. Describe the ECG.
2. What is your diagnosis?
3. Why is the patient hypotensive?
4. Which coronary vessel is likely to be involved?
5. How would you manage this patient?
6. What does the following ECG show?
A 21 year old male presents with palpitations. He brings with him a copy of his ECG recorded by his General Practitioner 3 weeks ago (A).At present he is on a cardiac monitor with P= 180, BP 100/60, Alert and orientated but feeling dizzy.
A
 B. The 12 lead taken in ED shows
B. The 12 lead taken in ED shows

A 21 year old male presents with palpitations. He brings with him a copy of his ECG recorded by his General Practitioner 3 weeks ago (A).At present he is on a cardiac monitor with P= 180, BP 100/60, Alert and orientated but feeling dizzy.
1. Describe ECG A.
2. Outline treatment plan for current attendance
3. Amiodarone is a commonly used antiarrhythmic agent,, what are its :
Mode of action
4 common side effects
One contraindication
A 74 year old female presents after waking at 5 am with sudden severe dyspnoea. SpO2 86% OA, afebrile. CXR shown below.

A 74 year old female presents after waking at 5am with sudden severe dyspnoea. SpO2 86% OA, afebrile. CXR shown below.
1. List 4 features shown on CXR
2. What is the diagnosis?
3. Explain by drawing or words Starling’s curve and how it might differ in this patient

The Frank–Starling law of the heart states that the stroke volume of the heart increases in response to an increase in the volume of blood filling the heart (the end diastolic volume) when all other factors remain constant. The increased volume of blood stretches the ventricular wall, causing cardiac muscle to contract more forcefully (the so-called Frank–Starling mechanisms)
Contractility can increase or decrease SV independent of LVEDP
4. Give 3 drugs with doses and routes you would use in this patient
5. What is the stimulus for releases of ANP and by what mechanism does it act?
A 75 year old female presents with recurrent syncope.

A 75 year old female presents with recurrent syncope.
1. Describe the ECG
2. List 4 common potential causes
3. The patient drops her BP to 70/30. How would you manage the patient?
45 year old male presents with 2 hour history of central crushing chest pain, sweaty and vomited twice. No PMH. On Oxygen, ongoing pain.

45 year old male presents with 2 hour history of central crushing chest pain, sweaty and vomited twice. No PMH. On Oxygen, ongoing pain.
1. What does the ECG show?
2. What is the diagnosis? What blood vessel is involved?
Acute MI, cause by proximal occlusion of LAD.
3. Give 4 management steps
4. Using the same ECG, the patient is a 76 year old man. PMH MI 3/12, 30min pain, now resolved, normal observations. Give 4 management steps
75 year old male presents having collapse, paramedics had difficult detecting pulse.
1. Describe the ECG, what is the diagnosis?

The patient has another ‘funny do’ in the ED, repeat ECG is below.
 2. Describe the ECG
2. Describe the ECG
3. How would you manage this patient?
4. What asystolic rhythm might he develop?
75 year old male presents having collapse, paramedics had difficult detecting pulse.
1. Describe the ECG, what is the diagnosis?
The patient has another ‘funny do’ in the ED, repeat ECG is below.
2. Describe the ECG.
3. How would you manage this patient?
4. What asystolic rhythm might he develop?
A 30 year old female presents with SOB and dizziness. Her blood pressure 80/40 mm Hg.

1. What is the diagnosis?
2. How would you manage this patient?
A 30 year old female presents with SOB and dizziness. Her blood pressure 80/40 mm Hg.
1. What is the diagnosis?
2. How would you manage this patient?
A 39 year old female presents with palpitations and collapse. Her BP on arrival is 95/55.
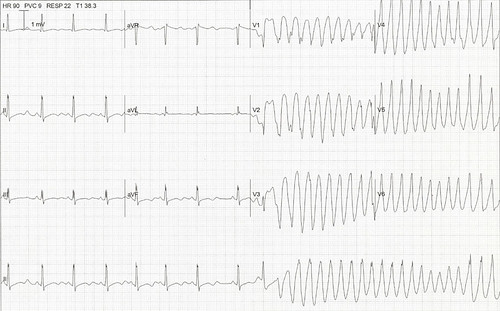 1. Describe the ECG, what is the diagnosis?
1. Describe the ECG, what is the diagnosis?
2. Give 3 possible causes
3. How would you manage this patient?
A 39 year old female presents with palpitations and collapse. Her BP on arrival is 95/55.
1. Describe the ECG, what is the diagnosis?
2. Give three possible causes
3. How would you manage this patient?
Further read: Lifeinthefastlane
Chest Pain of Recent Onset Nice 2010:
CHADS2 - The CHADS2 score is a clinical prediction rule for estimating the risk of stroke in patients with atrial fibrillation.
Score 0 aspirin; 1 aspirin or warfarin; 2 or more warfarin risk/benefit
Total marks: 23
Time allowed: 90 mins
Paper: Mallampati test as a predictor of laryngoscopic view
Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2010 Dec;154(4):339-43.
1. Provide a summary / abstract for the paper. (Up to 5 marks)
This should include all or some of the following points:
Aim. To determine the accuracy of the modified Mallampati test for predicting the difficulty of subsequent tracheal intubation.
Design. A cross-sectional, clinical, observational, non-blinded study. A quality analysis of anaesthetic care.
Setting. Operating theatres and department of anaesthesia in a university hospital in the Czech Republic.
Material and methods. Following local ethics committee approval and patients’ informed consent to anaesthesia, all adult patients (> 18 yrs) presenting for any type of non-emergency surgical procedures under general anaesthesia requiring endotracheal intubation were enrolled.
Prior to anaesthesia, Samsoon and Young"s modification of the Mallampati test (modified Mallampati test) was performed.
Following induction, the anaesthetist described the laryngoscopic view using the Cormack-Lehane scale. Classes 3 or 4 of the modified Mallampati test were considered a predictor of difficult intubation. Grades 3 or 4 of the Cormack-Lehane classification of the laryngoscopic view were defined as impaired glottic exposure.
The sensitivity, specificity, positive and negative predictive value, relative risk, likelihood ratio and accuracy of the modified Mallampati test were calculated on 2x2 contingency tables.
Results. Of the total 1,518 patients enrolled, 48 had difficult intubation (3.2%).
We failed to detect as many as 35.4% patients in whom glottis exposure during direct laryngoscopy was inadequate (sensitivity 64.4%).
Compared to the original article by Mallampati, we found lower specificity (82.4% vs. 99.5%), lower positive predictive value (0.107 vs. 0.933), higher negative predictive value (0.986 vs. 0.928), lower likelihood ratio (3.68 vs. 91.0) and accuracy (0.819 vs. 0.929).
Conclusion. When used as a single examination, the modified Mallampati test is of limited value in predicting difficult intubation in elective surgery patients.
2. Give three weaknesses of the study design and suggest improvements for these (up to 3 marks)
Strengths - there aren’t that many!
Weaknesses – there are lots of these!
The study could have been improved (for an EM readership) by:
3. Name one checklist which is useful in evaluating the quality of diagnostic papers such as this. Give two further questions / points within this checklist not covered by the weaknesses you have mentioned in question 2. above. (up to 3 marks)
Common checklists include QUADAS and STARD (see below)
The STARD statement can be found here (it is similar to QUADAS):
http://www.stard-statement.org/
In this study the “index test” is the Mallampati Score and the “reference standard” is the Cormack & Lehane Grade. You should go through this checklist with the study and see how many weaknesses you can now identify!
4. The table 3 below is taken from the results section.
 Summarise the results in the table in one sentence. What is the Mann-Whiney U test? (Up to 2 marks)
Summarise the results in the table in one sentence. What is the Mann-Whiney U test? (Up to 2 marks)
Men are taller and heavier than women!
The Mann Whitney U Test is a test used to compare continuous (or ordinal) data in two independent groups, when the data is non parametric (i.e does not follow a normal distribution). It is analogous to a t-test which does the same thing but for normally distributed data.
5. Construct a 2 x 2 table illustrating the main data from the current study (not Mallampati’s original). (Up to 2 marks)
| Actual Difficulty of Intubation(by Cormack Lehane Grade) | ||||
| Difficult (3/4) | Easy (1/2) | |||
| Predicted Difficulty of Intubation (Mallampati Class) | Difficult (3/4) | 31 | 258 | 289 |
| Easy (1/2) | 17 | 1212 | 1229 | |
| 48 | 1470 | 1518 | ||
6. Use your table in 5. above to demonstrate how the positive likelihood ratio and the accuracy were calculated. Explain how you would interpret the positive likelihood ratio in this study. (4 marks)
Positive LR = Sensitivity / 1 – Specificity
Sensitivity = a / a+c = 31 / 48 = 0.646
Specificity = d / b+d = 1212 / 1470 = 0.824
Positive LR = 0.646 / 0.176 = 3.67
Accuracy = total number (%) of “correct” predictions = a + d / a + b + c + d
Accuracy = 1243 / 1518 = 81.9%
LR+ above 10 means that a positive test (i.e. a higher Mallampati Score) will significantly increase the post test probability (of a difficult intubation) enough to make the test worth doing. Figures below 10 (like 3.67) mean that a positive test doesn’t really alter your chances of predicting the outcome enough to make it worth doing.
_Raslich_slika2.jpg?resize=618%2C152)

7. The authors used Fishers Exact Test to statistically compare their results with the results of Mallampati. Describe the indications for using this test as opposed to a Chi Squared Test? (Up to 2 marks)
The authors appear to have used 2 x 2 tables for each of the possible outcomes. An example for “true negative” is illustrated below.
| Study | ||||
| Adamus et al | Mallampati et al | |||
| Observed Result | True Negative | 1212 | 181 | 1393 |
| Not True Negative | 306 | 29 | 335 | |
| 1518 | 210 | 1728 | ||
Thus for box d (value 29), the expected value is 210 (the total column value) x 335 (the total row value) / 1728 (the overall total). This is 40.1. In this case all the expected values are greater than 10 and so Chi Squared could have been used. However, for some of the others (e.g. false positives), the expected values will be low so I suppose the authors went for Fishers Test for consistency!
8. What are your conclusions overall? Is this paper going to influence your practice? Briefly suggest any ideas for future research in this area? (Up to 2 Marks)
Overall this paper is not great and is unlikely to influence your practice. There are multiple weaknesses and potential areas of bias. In addition the results are very different from the original Mallampati Study.
The authors hint at the other factors which allow a good assessment of the airway (e.g. weight or patients etc..). A better study might look at the whole LEMON acronym which you are probably familiar with from ATLS. It could be done in an ED setting with independent assessment of LEMON and the final C&L grade / ease of intubation.
Finally given that the study results are so different from the original Mallampati Study you could propose some secondary research (a systematic review, Best BET or even CTR!) to answer the question posed.
Mallampati test as a predictor of laryngoscopic view. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2010 Dec;154(4):339-43.
A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985 Jul;32(4):429-34.